
Search results
Sponsored



During these unprecedented challenging times caused by the coronavirus CoVID-19 pandemic, we trust that you all stay safe and well and let the spirit of Ramadan remain in your hearts and light up your souls from within.
Directory:
Tags:

|


Directory:
Tags:

|


Directory:
Tags:
The leading killers in the United States are heart attacks and strokes. Annually, around 860,000 Americans die from heart disease or another untreated cardiovascular condition. The most preventable precursors to a heart attack are high blood pressure, bad nutrition habits, high cholesterol, smoking, limited or no physical exercise, obesity and type 2 diabetes.
Heart attacks and strokes are the leading causes of death in the United States. Every year, around 860,000 Americans die as a result of heart disease or another untreated cardiovascular condition. High blood pressure, poor nutrition, high cholesterol, smoking, little or
best cardiovascular specialist in NYC no physical activity, obesity, and type 2 diabetes are the most preventable precursors to a heart attack.
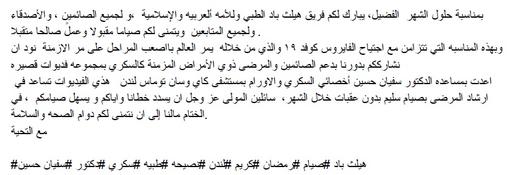
The onset of a heart attack can be sudden and severe, but most begin as a gradually increasing pain in your chest. In the United States, a heart attack occurs about once every 40 seconds. Strenuous activities like sports, heavy labor, and other physical activities are often credited as an inciting cause of a heart attack. But the real causes are typically longstanding health issues that are varied and complex.
Read more: https://newyorkcardiac.com/heart-attack
New York Cardiac Diagnostic Center
115 East 86th Street
New York, NY 10028
(212) 860–0796
Web Address: https://newyorkcardiac.com/
Our locations on the map:
https://g.page/Cardiologist-Upper-East-Side-NYC
https://plus.codes/87G8Q2JV+2G New York
Nearby Locations:
Upper East Side
Yorkville | Manhattan | Lenox Hill | Carnegie Hill | East Harlem
10028, 10075, 10128 | 10021 | 10029 | 10035
New York Cardiac Diagnostic Center
200 West 57th Street, Suite 200
New York, NY 10019
(212) 582–8006
Our locations on the map:
https://g.page/New-York-Cardiology-Midtown-NYC
https://plus.codes/87G8Q289+5Q New York
Nearby Locations:
Midtown
Hell`s Kitchen | Little Brazil | Lenox Hill | Diamond District
10019 | 10036 | 10021 | 10017
New York Cardiac Diagnostic Center
65 Broadway Suite 1806
New York, NY 10006
(212) 860–5404
Our locations on the map:
https://g.page/New-York-Cardiology-Downtown-NYC
https://plus.codes/87G7PX4Q+W2 New York
Nearby Locations:
Financial District / Wall Street
World Trade Center | Two Bridges | Tribeca | Lower East Side
10007 | 10002 | 10003, 10009
Working Hours:
Monday: 8 am — 5 pm
Tuesday: 8 am — 5 pm
Wednesday: 8 am — 5 pm
Thursday: 8 am — 5 pm
Friday: 8 am — 5 pm
Saturday: Closed
Sunday: Closed
Payment: cash, check, credit cards.
Directory:
Tags:
|



Directory:
Tags:

|

Directory:
Tags:

|

“If I’d known I was going to live this long I would have taken better care of myself.” Memorable words from Eubie Blake, the American jazz composer, lyricist and pianist who died in 1983 at the age of 96. Today, people do take better care of themselves. Examples of people who do, include rock legends Mick Jagger and Paul McCartney, the badboys of the 1960s who became the goodboys of the 1990s. Now, at 70 and 69 respectively, they continue to work, support worthy causes and enjoy a good quality of life.
Over the past 50 years, the number of people over 65 in the developed world has tripled and is projected to triple again by 2050. The UK’s Office of National Statistics forecasts that a third of babies born in 2012 will live to 100. “Age is uninteresting,” said Groucho Marx, “All you have to do is to live long enough.” Age, however has become interesting as it is an unavoidable part of the human condition and a significant challenge for nations where millions will be retiring with a third of their lives still ahead of them. They will no longer be productive, but will be in need of healthcare. Healthcare systems have been slow to adjust to the new realities of aging populations and the financial costs of treating the elderly.
One way for nations to manage retirement and aging was suggested by Euripides in 500BC. “I hate men,” he said, “who would prolong their lives by foods and charms of magic art, preventing nature’s course to keep off death. They ought, when they no longer serve the land, to quit this life and clear the way for youth.” Euripides’ sentiment resonates today. In advanced industrial economies there is a relatively low tolerance of elderly people. This is manifest in the number of offences against elderly vulnerable patients, which involves neglect and physical violence. In his 2013 Report into the UK's Mid-Staffordshire NHS Foundation Trust, where hundreds of patients had died as a result of inadequate care, Robert Francis said that between 2005 and 2009 patients were subject to, “appalling and unnecessary suffering”. In June 2012, at a conference in London’s Royal Society of Medicine, Professor Patrick Pullicino claimed that each year UK National Health doctors prematurely end the lives of about 130,000 elderly hospital patients because they are difficult to manage and to free up beds for younger patients.
According to a UN Report presented at the World Assembly on Aging in 2002, population aging is an unprecedented global phenomenon. The 21st century will witness more rapid aging than did the 20th century and countries that started the process later will have less time to adjust. There will be no return to the young populations of previous generations and aging populations will have profound implications for healthcare.
Moralists argue that healthcare is a human right and all people should be treated similarly unless there are sound moral reasons not to do so. But, who pays? Daniel Callahan, a contemporary philosopher widely recognized for his innovative studies in biomedical ethics has an answer. Invoking Euripides he argues that age should be a limiting factor in decisions to allocate certain kinds of health services to the elderly. The demographic shift, says Callahan, increases competition for scarce healthcare resources and therefore healthcare should be rationed. Life extending care for the over 70s should be replaced with less expensive pain relieving treatment. Opponents of rationing suggest that wealthy governments should reduce their defense spending and increase their commitment to healthcare and enact reforms to cut costs and improve the efficiency of healthcare systems.
Callahan, however, has little faith in political leaders to deliver cost cutting strategies and argues that calls to cut healthcare waste and inefficiency have been made for decades with no effect. This is definitely the case in the UK where subsequent governments have failed to reconcile escalating costs of healthcare with maintaining and improving the quality of care for the elderly. According to Callahan, “Our whole health care system is based on a witch’s brew of sacrosanct doctor-patient autonomy, a fear of threats to innovation, corporate and (sometimes) physician profit-making, and a belief that, because life is of infinite value, it is morally obnoxious to put a price tag on it.”
Some age related incurable diseases that affect mostly older people in wealthy countries have contributed to the ghettoizing of age. One such disease is Parkinson’s, a progressive degenerative neurological movement disorder, which affects between six and 10 million people worldwide. In the US, the combined direct and indirect costs of Parkinson’s disease is estimated to be nearly US$25 billion per year. Medication costs for an individual person with Parkinson’s is on average US$2,500 a year and therapeutic surgery, such as deep brain stimulation, can cost up to US$100,000 dollars per patient.
However, not all age related diseases are like Parkinson’s. Indeed, it is not altogether true that old age corresponds to debilitating diseases and hikes in healthcare costs. Indeed, healthy years among the elderly are increasing and the spike in health costs tend to be in the last two years of life, regardless whether a person is 99 or nine. Rather than viewing the elderly as a burden and assessing them by their chronological age, it might be more appropriate to view them as assets and assess them by their number of healthy years. Healthy years are not necessarily years without illness, but years in which people manage whatever medical conditions they might have. A good example of this is Dame Maggie Smith, the English film, stage and television actress, who at the age of 78 has recently won a Golden Globe Award for her role as the Dowager Countess of Grantham in the television series Downton Abbey.
Longevity is one of the greatest successes of 20th century medical science and nutrition, but its challenges include the dearth of health workers with geriatric skills, the prevention of physical disabilities and the extension of healthy years. Recent studies suggest that healthy aging is possible and chronic non communicable illnesses such as heart disease, diabetes and dementia, may be delayed or prevented by certain lifestyle choices. Notwithstanding, currently there are millions of elderly people who have not taken good care of themselves and require specialist geriatric care.
In the US there is a monetary disincentive for doctors to specialise in geriatrics since geriatricians earn significantly less per year than more mainstream specialists. Further, only 11 of the 145 US medical schools have fully fledged geriatric departments. In 2010 the US federal budget allocated $11 million to fund geriatric education. Interestingly, today a substantial amount of geriatric care in wealthy countries is undertaken by health professionals trained in poorer countries. This raises ethical questions about rich countries encouraging the immigration of health workers from countries that lack them and the responsibilities of migrant health professionals to countries of their origin. Although geriatricians in the UK are well compensated, the British Geriatric Society reports that the number of geriatricians is not keeping pace with the needs of geriatric care.
According to the OECD between 10% and 20% of populations in developed economies require long term care and costs between 1% and 2% of GDP and these costs are projected to increase. The costs of long term care are skewed because a significant proportion of elderly care is carried out by informal, unpaid carers who are often family members. For example, in the UK there are 1.5 million official carers and about 5 million unpaid carers. In the developing world the situation is more extreme and some 60% of people over the age of 60 live with their children or grandchildren. While familial care may yield significant benefits, it is not a long term solution because as developing economies become more westernized, their family structures become more nuclear and less able to provide the support and care that they do now.
According to the first noble truth of Buddhism, life is painful and involves suffering. For a significant proportion of elderly people this is certainly the case, but it need not be. On an individual level, living longer must be welcome, but more generally, the greying of populations is perceived in terms of increased costs and pressure on overstretched healthcare systems, rather than freeing-up valuable resources that may contribute to society. Although elderly people tend to have long term medical conditions, increasingly they are successfully managed to allow a good quality of life. Old age is not a disease. Elderly people are a valuable resource of intellectual capital and knowhow, which nations cannot afford to waste. Unlocking this reservoir of grey-knowledge is important for the future wealth of nations. Let us hope nations have something better to offer their elderly than to call on them to do as Captain Oates did on the 16th March 1912. On his return from the South Pole, Oates, convinced that his ill health compromised his comrades, walked from his tent into a blizzard saying, "I am just going outside and may be some time.” He was never seen again.
Whose age is it anyway?
Directory:
Tags:

|


Publications by Dr Matthew Banks
Reviews
Banks MR
Should patients expect their colonoscopy to reach the standards experienced by bowel cancer screening patients?
Frontline Gastroenterol 2012;3:122-123
Mannath J, Banks MR
Emerging technologies in Endoscopic Imaging
F1000 Med Rep. 2012;4:3. Epub 2012 Feb 1.
Kent A & Banks MR
Functional Gastrointestinal Disorders: Diarrhea
Gastroenterology Clinics of North America. Hunt (eds),
Sept 2010;39(3):495-507
Banks M.
The modern investigation and management of gastro-oesophageal reflux disease. Clinical Medicine
2009;9(6):1-5
Burleigh DE & Banks MR
Stimulation of intestinal secretion by vasoactive intestinal peptide and cholera toxin. Autonomic Neuroscience.
2007;133(1):64-75
Farthing MJG, Casburn-Jones A, Banks MR
Diarrhoea. Prescriber 2003;14 (20):48-59.
Farthing MJG, Casburn-Jones A, Banks MR.
Getting control of intestinal secretion: thoughts for 2003.
Digestive and Liver Disease 2003;35:378-385
Banks MR, Farthing MJG.
Fluid and electrolyte absorption. Current Opinion in Gastroenterology 2001;
18 (2): 176-181.
Banks MR, Farthing MJG.
Current management of Acute Diarrhoea. Prescriber 2001;
12(12):83-93.
Banks MR, Farthing MJG.
The Management of Acute Diarrhoea. Prescriber 2000;
11(4): 97-105
Case reports
Pasha Y, Banks M.
Medical mystery: an unusual cause of anaemia
Br J Hosp Med (Lond). 2010 Feb;71(2):113.
Pasha Y, Pickard L, Cohen P, Banks MR
An unusual endoscopic diagnosis for acute epigastric pain
Scand J Gastro 2008;43(9):1151-2.
Pasha Y, White WJ, Chew NS, Banks M.
The importance of never ignoring an unexplained metabolic acidosis. Incarcerated femoral hernia. QJM.
2008 Oct;101(10):825-6. Epub 2008 Aug 28.
Green L, Banks MR
HIV associated encephalopathy, a grey case. Int J STD’s AIDS.
1995; 6: 744
Original papers
Radiofrequency ablation for early oesophageal squamous neoplasia: Outcomes form United Kingdom registry.
Rehan J Haidry, Mohammed A Butt, Jason Dunn, Matthew Banks, Abhinav Gupta, Howard Smart, PradeepBhandari, Lesley Ann Smith, Robert Willert, Grant Fullarton, Morris John, Massimo Di Pietro, Ian Penman, Marco Novelli, Laurence B Lovat
World Journal of Gastroenterology 09/2013; 19(36):6011-6019. 2.47
Radiofrequency Ablation (Rfa) And Endoscopic Mucosal Resection For Dysplastic Barrett’s Esophagus And Early Esophageal Adenocarcinoma: Outcomes Of Uk National Halo Rfa Registry.
R J Haidry, J M Dunn, M A Butt, M Burnell, A Gupta, S Green, H Miah, H L Smart, P Bhandari, L Smith, R Willert, G Fullarton, M Di Pietro, C Gordon, I Penman, H Barr, P Patel, P Boger, N Kapoor, B Mahon, J Hoare, R Narayanasamy, D O’Toole, E Cheong, N C Direkze, Y Ang, M Novelli, M R Banks, L B Lovat
Gastroenterology. 2013 Mar 28.doi:pii: S0016-5085(13)00459-9. 10.1053/j.gastro.2013.03.045
Wallace MB, Crook JE, Saunders M, Lovat L, Coron E, Waxman I, Sharma P, Hwang JH, Banks M, DePreville M, Galmiche JP, Konda V, Diehl NN, Wolfsen HC. Multicenter, randomized, controlled trial of confocal laserendomicroscopy assessment of residual metaplasia after mucosal ablation or resection of GI neoplasia in Barrett’s esophagus. GastrointestEndosc. 2012 Sep;76(3):539-47.e1. doi: 10.1016/j.gie.2012.05.004. Epub 2012 Jun 28
Dunn JM, Mackenzie GD, Banks MR, Mosse CA, Haidry R, Green S, Thorpe S, Rodriguez-Justo M, Winstanley A, Novelli MR, Bown SG, Lovat LB. A randomised controlled trial of ALA vs. Photofrin photodynamic therapy for high-grade dysplasia arising in Barrett’s oesophagus. Lasers Med Sci. 2012 Jun 15.
Banks MR, Haidry R, Butt MA, Whitley L, Stein J, Langmead L, Bloom SL, O’Bichere A, McCartney S, Basherdas K, Rodriguez-Justo M, Lovat LB. High resolution colonoscopy in a bowel cancer screening program improves polyp detection. World J Gastroenterol. 2011 Oct 14;17(38):4308-13.
Dunn JM, Banks MB, Oukris D, McKenzie GD, Thorpe S, Winstanly A, Novelli MR, Bown S, Lovat LB. Radiofrequency ablation is an effective treatment for high grade dysplasia in Barrett’s esophagus after failed Photodynamic therapy – a case series. Endoscopy. 2011 Jul;43(7):627-30
Dunn JM, Mackenzie GD, Oukrif D, Mosse CA, Banks MR, Thorpe S, Sasieni P, Bown SG, Novelli MR, Rabinovitch PS, Lovat LB. Image cytometry accurately detects DNA ploidy abnormalities and predicts late relapse to high-grade dysplasia and adenocarcinoma in Barrett’s oesophagus following photodynamic therapy. Br J Cancer 2010 May 25;102(11):1608-17
Kent AJ, Graf B, Prasad P, Banks M, Feher M. Diabetes Treatments, Gastrointestinal Symptoms and lower Gastrointestinal Endoscopy. Br J Diabetes &Vasc Dis 2009; 9: 129
Banks MR, Farthing MJG, Robberecht P, Burleigh DE. Anti-secretory actions of a novel vasoactive intestinal polypeptide (VIP) antagonist. British J Pharmacol 2005; 144: 994-1001.
Banks MR, Golder M, Farthing MJG, Burleigh DE. Intracellular potentiation between two second messenger systems may contribute to cholera toxin-induced intestinal secretion in humans.GUT 2004;53:50-57
Mulcahy HE, Kelly P, Banks MR, Connor P, Patchet SE, Farthing MJG, Fairclough PD, Kumar PJ. Factors Associated with Tolerance to, and Discomfort with, Unsedated Diagnostic Gastroscopy.Scand J Gast 2001; 36: 1352-1357
Banks MR, Kumar PJ, Mulcahy HE. Pulse Oximetry saturation levels during routine unsedated diagnostic upper gastrointestinal endoscopy.Scand J Gast 2001; 36: 105-109.
Pollock RCG, Banks MR, Fairclough PD, Farthing MJG. Dilutionaldiarrhoea – underdiagnosed and over-investigated.Europ J GastHep. 2000; 12: 1-3
Rockall AG, Lamb GM, Banks MR, Barrett SP, Al-Kutoubi MA. A prospective study of bacteraemia and bacterial contamination rates of catheters and wires during angiography.JInterventRadiol 1997; 12; 107-111.
